


How the FDA failed America by pushing approval for the COVID vaccine for children, ignoring danger signals, over protests and resignations from its own leadership

I have a COVID op-ed coming out soon, and I have been moving to a new apartment. Apologies for the lull in articles. Here is an article about the COVID-19 vaccine and myocarditis to tide you over. Be back soon. - Kevin
An article by Zachary Brennan at Endpoints released emails by Marion Gruber, a top official and Director of Vaccines Research and Safety who resigned after 32 years at the FDA, where she cited concerns with the accelerated approval of the vaccine for young people.

Where is the evidence on myocarditis and the vaccine today?
First, misinformation about vaccines is being pushed by all sides.
From the public health community, our leaders, and the media, the benefits of the COVID vaccine have been constantly exaggerated.
For example, see these false claims from people who, at the time, knew better.




These public figures made these claims because they thought that making them would encourage people to get vaccinated. They distorted the science in order to encourage behavior that they thought was beneficial, and because they were under political pressure.
They told "noble lies".
*I* believe that people should be armed with all of the information to make their own decisions. Not fear or propaganda.
I believe that the scientific authorities should be providing this information. I will do what they *should* be doing.
That is why I am writing this article.
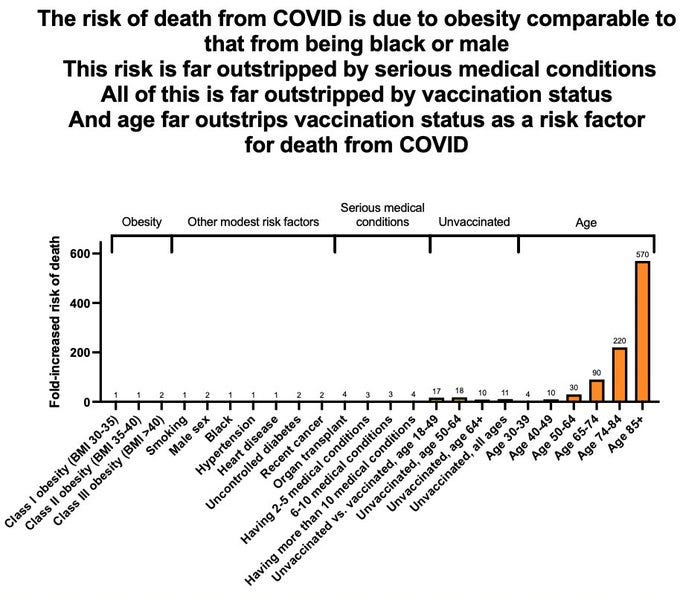
Let's start with the GOOD things about the COVID vaccine: it protects from death and severe disease from COVID.
These data aren't perfect, but they put into perspective, very roughly, the benefits of vaccination.
References: https://nature.com/articles/s41586-020-2521-4 https://cdc.gov/pcd/issues/2021/21_0123.htm https://cdc.gov/mmwr/volumes/70/wr/pdfs/mm7037e1-H.pdf
Now let's look at the same exact graph, but with age added.
It blows everything else away.
Age is by far the largest risk factor for COVID death, massively outstripping even vaccination status or any other risk factor.
Indeed, the risk of death from COVID has been recently estimated to be as high as 15% among people aged 85 or older.
That is, 1-in-7 unvaccinated people aged 85 or older die from being infected by COVID-19.

Let's go back to the first graph I posted to see what the impact of vaccination would be on that risk.
That turns into about 1-in-70 with the vaccine. That's a huge boost in survival!
That's why it is so important for older people and people at high risk to get vaccinated.

Here's the problem with the COVID vaccine. The risk of harm from the vaccine goes up as you get younger, while the risk of harm from COVID goes up as you get older.
It looks something like this.

So, at some point the risk of harm could be higher for the vaccine than for COVID!
And the scientific fact is, at the present moment, we don't yet know if that is the case.
Let's take a look at the evidence.
In this paper, the risk of myocarditis is much higher from the Moderna vaccine than it is from COVID for men under the age of 40. (For the Pfizer vaccine, it is a dead heat.)

Reference: https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.122.059970
This is why, you will remember, recommendations for young men pivoted away from Moderna toward Pfizer.
But not before millions of men took the second dose of the Moderna vaccine.
But here is for the Pfizer vaccine for adolescents:
"Among 12-17-year-olds, two-dose vaccination was uniformly favourable only in nonimmune girls with a comorbidity. In boys with prior infection and no comorbidities, even one dose carried more risk than benefit"

Now check out this graph from the above paper. It summarizes all studies looking at how many hospitalizations were prevented by the second dose of the vaccine (blue bars), versus all studies looking how many cases of myocarditis were caused by the vaccine (red bars).
What's interesting is that most of the red bars are longer than most of the blue bars.
Meaning there is likely more myocarditis from the second dose of the vaccine than there is from COVID19.
This is definitely true for omicron and those without comorbidities.

This is because there is almost no myocarditis from COVID during omicron.
Arguably, myocarditis does not occur with COVID anyway.
It would seem therefore that the second dose of the vaccine is worse than COVID-19 is and that therefore the second dose of the vaccine should be avoided in adolescent males.
There are arguments against this interpretation.
One is that, although myocarditis might be much more common in those adolescent males given the second dose of the vaccine, myocarditis from COVID-19 is much worse than from the vaccine.
This does not hold up for a few reasons.
As Anish Koka has argued, the myocarditis in children due to COVID may not even be real myocarditis, while the vaccine-induced myocarditis certainly is.

Anish is referring to this recent study that compares the troponin levels from "myocarditis" in MIS-C with classic myocarditis to vaccine-induced myocarditis.
No troponin elevation = no heart muscle damage.
Reference: https://www.ahajournals.org/doi/10.1161/JAHA.121.024393
And to be clear, heart muscle damage is irreparable: heart muscle cells do not regenerate. Once they die, they do not grow back. The damage to the heart is permanent.
Things get more interesting. Using cardiac MRI, there is a metric called the late gadolinium enhancement (LGE) that visualizes scarring of the heart due to damage.

Reference: https://radiopaedia.org/articles/late-gadolinium-enhancement-2?lang=us
This case study shows "extensive LGE" post-COVID vaccination.

Extensive heart damage and scarring!
This is confirmed by a new study published by the Lancet in a larger cohort:
At 3-6 months after myocarditis due to the COVID-19 vaccine in children and young adults, heart abnormalities remain in more than 50%!

Reference: https://www.thelancet.com/journals/lanchi/article/PIIS2352-4642(22)00244-9/fulltext
Indeed, at 3-6 months, 13% of those with vaccine-induced myocarditis had evidence of ongoing inflammation of the heart and unresolved myocarditis!
A full 47% of 151 who received cardiac MRI had LGE, which, again, is an indication of heart muscle damage and scarring.
We do not know what the long-term consequences of this heart damage are. However, it is possible that it ultimately may make the heart more vulnerable, so that heart attacks, heart failure, and other cardiac events may be more severe in people with this long-term damage.
We have case studies indicating exactly this.
This recent one is disturbing and shows permanent heart dysfunction after the COVID vaccine.



Marty Makary, a physician and professor at Johns Hopkins, writes scathingly


To what degree do other people who have experienced myocarditis experience permanent symptoms like this? How long do they take to manifest?
We don't know.
And that's the problem. This issue was well-known during the review process at the FDA. It led to the resignation of the director of the Vaccine Reviews and Safety and her deputy.
Yet approval was bulldozed through. Safety was not the highest priority.


The problem with vaccine-induced myocarditis is not necessarily that it is a public health problem that undermines the utility of the vaccine (though it may). Rather, the problem is that so many open questions remain about the risk-benefit analysis of the vaccine, yet it was still approved.
It points to a fundamental institutional failure inside the FDA, which buckled to political pressure.
As a result, we have the current situation. The vaccine may be useful in children. It may be that, despite the risk of myocarditis, other benefits are so extensive that the myocarditis risk is outweighed.
But we don't know. And the credibility of the vaccine for children--and FDA's credibility--is in question. FDA has only itself to blame.
I have been sent many studies and speculations for why the COVID vaccine's benefits outweigh its risks for children and adolescents, but the fact is that, without the actual studies, we simply don't know.
Science requires evidence, not speculation.
And the FDA and CDC, and those who defend the FDA and CDC's current recommendations are failing science.
You write the vaccine "protects from death and severe disease from Covid." But the indicator trial for Pfizer showed a fourfold increase in all-cause mortality (table S5). And the CDC's problematic definition of "severe covid" is either: hospitalization, admission to ICU, intubation, or death combined with a positive nucleic acid test. So you can have "severe covid" if you get hit by a truck or have a heart attack and have a positive nucleic acid test. At most, the trial data shows the injection negatively correlates with the chance you will have a positive nucleic acid test when you get admitted to the hospital for something that is not necessarily caused by the presence of the molecular sequences amplified on that test. That's not proof of protection from severe disease. Measured on the key clinical endpoint of death, the "vaccine" has negative 400% efficacy.
All these studies hinge on the validity of nucleic acid testing, which is a surrogate marker that has failed to validate - that's why you get all these "covid cases" of healthy people diagnosed with a lab test.
Since my Twitter is still not back, and you asked which book you should read on Twitter -read 1984. It's a fascinating book by a fascinating person.
https://eharding.substack.com/p/three-types-of-dystopian-novels